
Why I Rejected Typical Lactate Threshold Testing
Three reasons I decided to offer Singapore's first advanced lactate testing service.

I just launched my lactate threshold testing service, and it looks different from what other local providers offer.
Consequently, I have received many questions.
I am therefore writing a series of articles to show how these differences lead to drastically superior outcomes, starting with this piece.
Upcoming articles in this series include:
Reasons Heart Rate Zones Are Deprioritised in Your Lactate Threshold Report
Better Menopause Weight Management Through Advanced Lactate Testing
Why Body Composition Matters in a Lactate Threshold Test
Etc.
With that, let’s get started.
How Typical Lactate Testing Is Done
In Singapore’s market, this is the most common testing protocol you’ll see:
Drawing blood as you run at increasing intensities
Plotting a curve of the lactate readings
Identifying the point where lactate began to rise — usually set at 2 and 4 mmol/L.
You will then receive your training zones.
However, this is a flawed process, and many world-class organisations, such as national sport federations, have already moved away from it.
Below, I list three easy-to-understand explanations.
(Let me know if you’d also like me to deep-dive into the more technical justifications.)
1. How the Typical Process is Physiologically Flawed
The first reason revolves around the two pre-determined points, 2 and 4 mmol/L.
They were originally proposed by Mader et al. (1976) to define the aerobic and anaerobic thresholds, respectively.
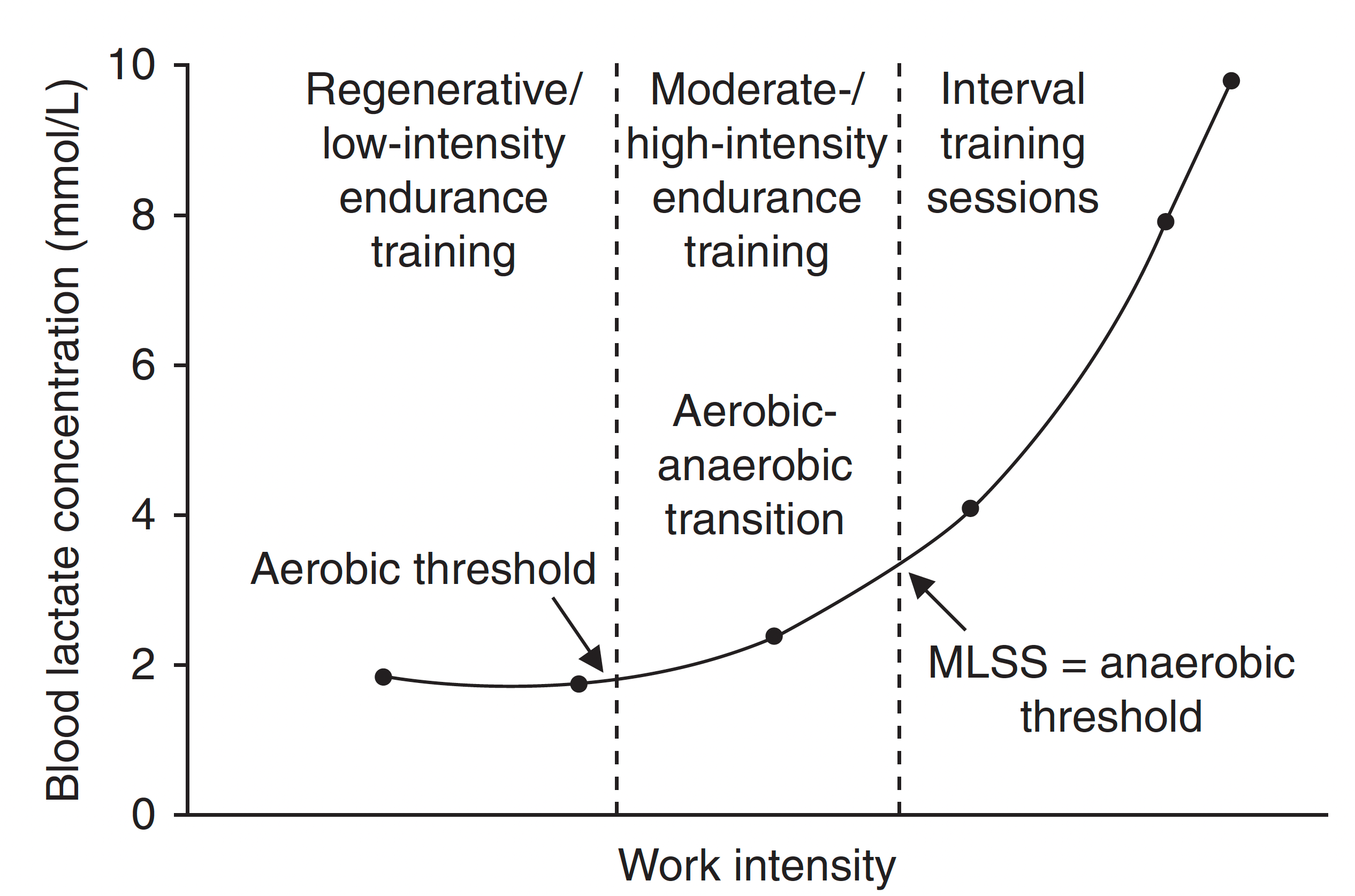
However, this approach has limitations.
A fundamental problem is that blood lactate responses are highly individual.
Endurance athletes, for example, often have an anaerobic threshold above 4 mmol/L.
For non-athletes, who are likely less conditioned, this anaerobic metabolism may occur at 2.8 mmol/L.
Applying universal cutoffs of 2 and 4 mmol/L ignores this physiological reality (Heck et al., 1985; Faude et al., 2009).
Consequently, the training zones you derive using such methods may be skewed.
The protocol may also lead to advice that makes you slower and/or misguides your health training priority — more on that in the ‘incomplete training guidance’ section of this article.
2. How the Typical Process Costs More
Yes, you read that right. The typical process is more expensive, less comprehensive, and still the most frequently practised.
For instance, you might realise these common limitations in the local market:
1. VO2 Max and lactate threshold tests require separate effort
2. Doing both tests means additional costs
3. The training zones derived from clinical-grade VO2 Max and Lactate Threshold tests differ
From a protocol perspective, you might also have to compromise if you want to do both a lactate threshold test and a VO2 Max test concurrently.
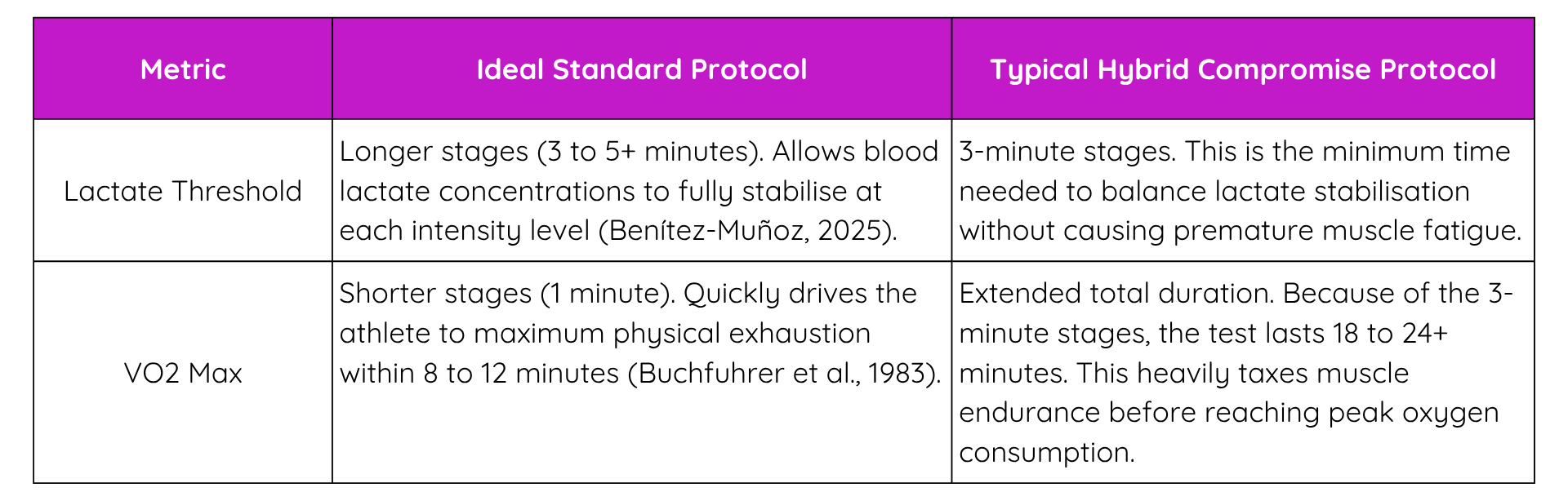
The typical testing processes are not optimal in terms of cost, effort, and results.
It is partly why I opted for a testing service that lets you get VO2 Max and advanced Lactate Threshold metrics in a single effort, at no additional cost and with fewer compromises.
3. How the Typical Process Provides Incomplete Training Guidance
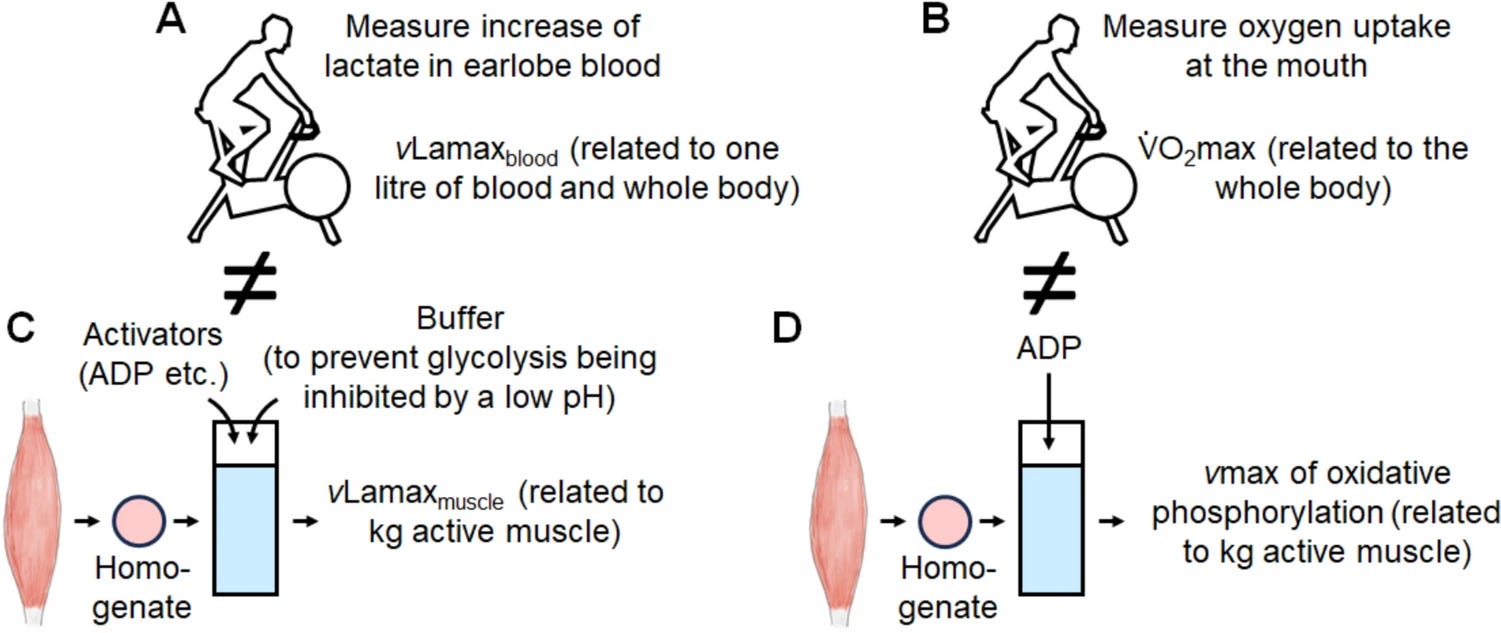
An important health and sports metric that is often missing from typical lactate assessments is VLaMax.
i.e. Maximum Lactate Accumulation Rate
It reflects how quickly your muscles produce lactate.
Loosely put, VO2 Max measures your aerobic system’s capabilities, and VLaMax is the equivalent for your anaerobic system (Quittmann, 2026).
Knowing your VLaMax changes how you train for your health and sporting goals.
For example,
Case 1: Someone focused on health might train for a higher VO2 max, but after understanding their VLaMax, the training focus might shift to tweaking the latter instead.
Case 2: An athlete training for HYROX would want a higher VLaMax compared to a marathon runner, even though both would train for a higher maximum lactate steady state.
Case 3: Both general classification cyclists and classic specialists might aim for higher VO2 max and LT2, but have differing VLaMax goals due to the nature of their event.
The list of examples goes on to include other activities, such as triathlon and team sports.
Without advanced metrics like VLaMax, your training recommendation from a typical lactate threshold test might distract from your training priority and, in some cases, even lead you away from your goal.
And VLaMax is only one of the many metrics that typical tests miss.
I will cover more of such cases in a future article; you can then better understand how VLaMax and other metrics, such as FatMax and CarbMax, more accurately inform your health and sports fuelling recommendations.
For now, I hope it is clear to you that the typical lactate threshold test provides incomplete information for tweaking your training compared to the one my company offers.
Conclusion
My next article focuses on why heart rate zones, typically used in lactate threshold reports, are deprioritised by my company.
If you are interested in learning more, please consider subscribing to the newsletter.
Get in touch for a chat if you are interested in my team’s physiological testing services.
Till next time, take care!
References
Benítez-Muñoz, J. A. (2025). Factors influencing blood lactate concentration during exercise: A narrative review with a lactate shuttle perspective. Acta Physiologica, 241(12), e70131. https://doi.org/10.1111/apha.70131
Buchfuhrer, M. J., Hansen, J. E., Robinson, T. E., Sue, D. Y., Wasserman, K., & Whipp, B. J. (1983). Optimizing the exercise protocol for cardiopulmonary assessment. Journal of Applied Physiology: Respiratory, Environmental and Exercise Physiology, 55(5), 1558–1564. https://doi.org/10.1152/jappl.1983.55.5.1558
Faude, O., Kindermann, W., & Meyer, T. (2009). Lactate threshold concepts: How valid are they? Sports Medicine, 39(6), 469–490. https://doi.org/10.2165/00007256-200939060-00003
Heck, H., Mader, A., Hess, G., Mücke, S., Müller, R., & Hollmann, W. (1985). Justification of the 4-mmol/l lactate threshold. International Journal of Sports Medicine, 6(3), 117–130. https://doi.org/10.1055/s-2008-1025824
Mader, A., Liesen, H., Heck, H., Philippi, H., Rost, R., Schürch, P., & Hollmann, W. (1976). Zur Beurteilung der sportartspezifischen Ausdauerleistungsfähigkeit im Labor [Assessment of sport-specific endurance capacity in the laboratory]. Sportarzt und Sportmedizin, 27, 80–88, 109–112.
Mavroudi, M., Chaouachi, A., Chaouachi, M., & Haddad, M. (2023). Blood lactate and maximal lactate accumulation rate at three sprint swimming distances in highly trained and elite swimmers. Sports, 11(4), 87. https://doi.org/10.3390/sports11040087
Pacitti, L. J., Shikaze, K. E., Simpson-Stairs, N., Stringer, J., & Gurd, B. J. (2025). Individual variability in lactate response to cycling prescribed using physiological thresholds and peak work rate: A crossover within-participant repeated measures study. European Journal of Applied Physiology, 125(7), 1797–1807. https://doi.org/10.1007/s00421-025-05711-7
Quittmann, O. J. (2022). Lactate thresholds and the simulation of human energy metabolism during exercise. Frontiers in Physiology, 13, 899670. https://doi.org/10.3389/fphys.2022.899670
Quittmann, O. J. (2026). Maximal lactate accumulation rate (ċLamax): Current evidence and future directions for exercise testing and training. European Journal of Applied Physiology, 126(1), 1–36. https://doi.org/10.1007/s00421-025-06022-7
Wackerhage, H., Kabasakalis, A., Seiler, S., & Heck, H. (2025). Is the VLAMaX for glycolysis what the VO2 Max is for oxidative phosphorylation? Sports Medicine, 55(8), 1853–1866. https://doi.org/10.1007/s40279-025-02259-6