
Singapore’s First Lactate Threshold Test for Menopausal Weight Management
Evidence-based metabolic profiling for women navigating the menopause transition.

There is a weight management test for women going through the menopause transition that doctors in Singapore have been missing out on.
Perhaps because it wasn’t available in Singapore until my company recently started offering it.
I’m referring to an advanced lactate threshold test, which provides insights that a typical one does not.
E.g. FatMax, CarbMax, VLaMax
These metrics, in short, help you formulate what exact cardiorespiratory exercises you should do, inform you how your diet is affecting your physiology, etc.
Results aside, the test protocol my company uses is also friendlier for non-athletes, making it valuable to the general population.
For more educational content about my company’s advanced lactate threshold test, check out this link.
With that said, let’s dive into how my company’s test will benefit your weight management journey.
1. It Measures the Fat-Burning Capacity the Menopause Transition Erodes
Before menopause, women rely more on fat as a fuel source during exercise than men at the same relative exercise intensity (Tarnopolsky et al., 1990; Venables et al., 2005).
This is because estrogen promotes fatty-acid uptake and oxidation in skeletal muscle (Isacco et al., 2012).
As those levels decline, that advantage fades.
Research shows that this shift is measurable:
Postmenopausal women had approximately 33% lower whole-body fat oxidation during exercise than premenopausal women. Importantly, correction for lean body mass (LBM) reduced this difference to approximately 23%, indicating that much of this difference is attributable to lower lean body mass rather than to a direct hormonal effect alone (Abildgaard et al., 2013).
A separate longitudinal study also found fat oxidation fell by 32% in women who became postmenopausal over a four-year follow-up.
Quantifying fat oxidation early, therefore, matters, so you can use exercise interventions to better optimise your fat oxidation capacity.
That’s where my company’s test comes in.
It can tell you your maximal fat oxidation (MFO) and the exercise intensity at which it peaks (FatMax) — giving you a clear baseline for the metabolic system the transition affects most, and a way to track whether training is preserving or restoring it.
2. It Helps You Better Manage Your VO₂ Max — One of the Most Important Health Numbers at Midlife
Cardiovascular disease (CVD) is the leading cause of death globally among women (Vogel et al., 2021), and one way to track your cardiovascular health is to measure your VO₂ Max — how much oxygen your body can utilise during maximal exercise.
A meta-analysis of 33 studies pooling data from over 100,000 participants found each 1-MET (3.5 ml/kg/min) increase in aerobic capacity was associated with a 13% lower risk of all-cause mortality and a 15% lower risk of cardiovascular events (Kodama et al., 2009).
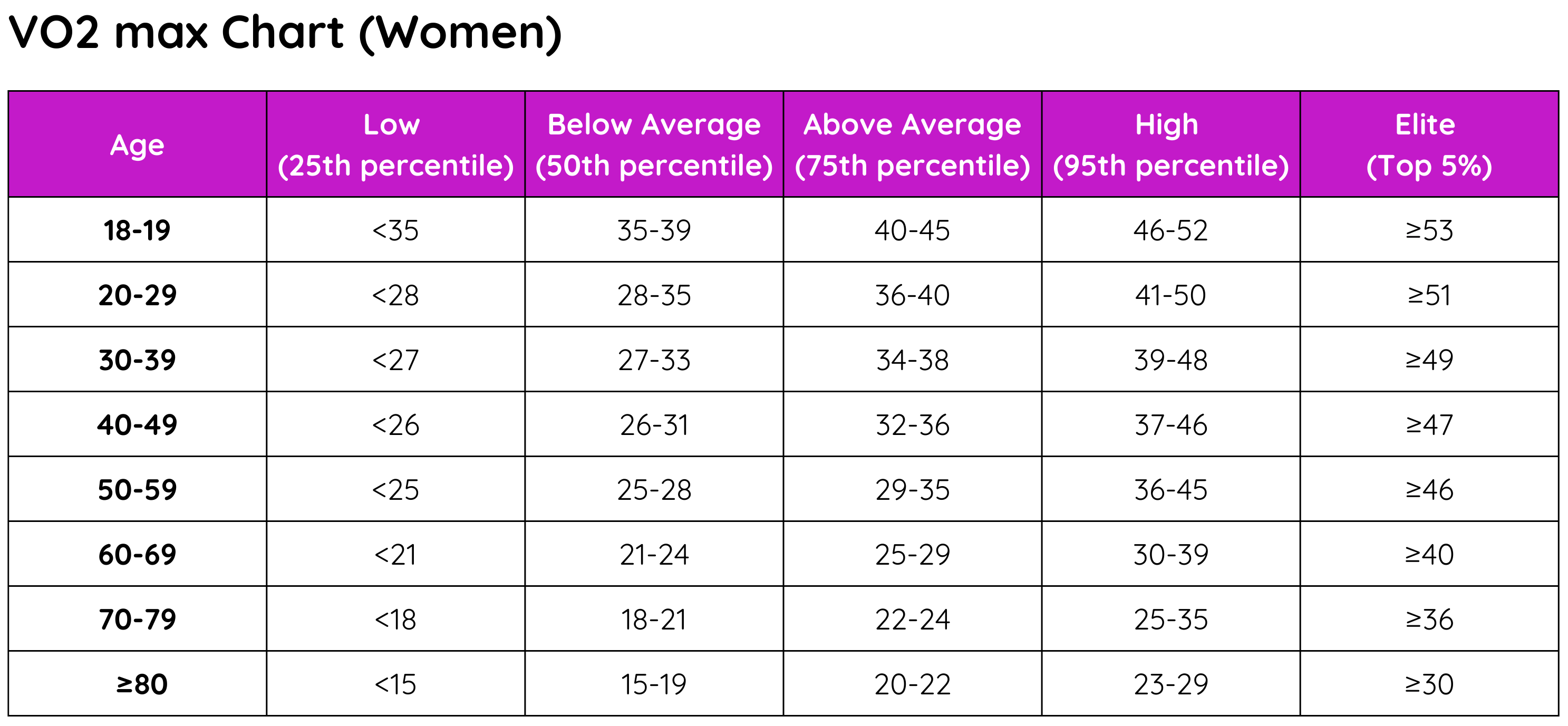
For reference, here’s the VO2 Max Chart for women, in units of ml/kg/min.
VO₂ Max declines with age — at roughly 10% per decade after age 25–30 — and the rate of decline can accelerate in sedentary women after menopause (Fleg et al., 2005).
In the context of weight loss and exercise recommendations, however, knowing your VO₂ Max from a VO₂ Max test alone often falls short, as the results may not be fully actionable on their own.
They do not tell you whether optimising for your VO₂ Max should be a priority, or whether other metabolic parameters warrant more urgent attention.
That’s where a comprehensive lactate threshold test comes in — to provide you with a clearer picture of what exactly happens when you exercise at different intensities, and consequently, what your action plan should be.
3. It Informs You About Your Maximal Glycolytic Rate (VO2 Max’s Sister Metric)
Not all lactate threshold tests measure maximal glycolytic rate (VLaMax), but my company’s does.
The metric is important for women undergoing the menopausal transition because a higher VLaMax shifts fuel use toward carbohydrate and lowers fat oxidation at submaximal intensities — thereby suppressing the very fat oxidation that the estrogen decline is already eroding (Mader & Heck, 1986; Randle et al., 1963).
So deliberately raising VLaMax makes sense only if you are training for a genuinely glycolytic event (such as HYROX, a team sport, or high-intensity interval training).
For most women in the menopausal transition, the aim is to keep VLaMax moderate to low so fat oxidation stays high — and knowing where you stand lets you train toward that.
4. It Customises Your Cardiorespiratory Exercise Recommendations
Cardiorespiratory exercise recommendations are often prescribed in the form of varying training intensities, also called training zones.
One way to define these zones is to base them on percentages of your maximum heart rate.
However, the method poorly reflects any individual’s actual physiology, and research has demonstrated that it routinely misclassifies exercise intensity (Iannetta et al., 2020).
To add to that, heart rate can also be an unreliable guide in midlife women — affected by hormonal fluctuations, sleep disruption, hot flushes, or medication.
This also means that typical lactate threshold tests that give you training zones based on heart rate fail to address relevant pitfalls.
These are the areas where my company’s differentiation matters.
We set your training zones from actual metabolic events: the lactate threshold, the maximal lactate steady state (MLSS), FatMax, and the fat-to-carbohydrate crossover point.
This means your training recommendation will be time spent at the intensity (e.g. pace) that actually delivers the intended physiological adaptation — whether the goal is building aerobic base, improving metabolic flexibility, or improving cardiovascular fitness.
5. It Tracks Body Composition — and Whether Resistance Training Is Working
During the menopausal transition, fat mass gain accelerates — the rate of fat gain approximately doubles at the onset of perimenopause (Greendale et al., 2019) — with the increase directed predominantly toward visceral abdominal fat (Lovejoy et al., 2008).
Simultaneously, lean mass begins to decline during the transition. Both trends continue for approximately two years after the final menstrual period, after which fat and lean mass trajectories stabilise (Greendale et al., 2019).
Resistance training is an effective tool to counter these changes. Evidence shows combined resistance plus cardiorespiratory (aerobic) training tends to produce the broadest benefits for cardiovascular health and body composition (Ioannidou et al., 2024).
Related article: Three Types of Strength Training For Menopause
Again, this is where my company offers something that other providers typically do not.
Body composition reporting is included in my company’s lactate threshold test (because it should be).
And the test serves as a check to ensure your muscle health is properly addressed whenever you come in for an assessment.
Sneak peek: one of my company’s upcoming upgrades is a body composition analysis more accurate than the current gold-standard DEXA (and physiological testing clients will get to use it for free, i.e. a $300+ cost saving)
6. It Creates a Baseline and a Feedback Loop
Establishing MFO, VO₂max, fat-free mass, and lactate thresholds now, then retesting every few months, shows you whether the current training and nutrition strategy is working — and allows for course correction before months are lost.
For example:
A rising or stable VO₂max, with preserved fat-free mass and improved fat oxidation capacity, is a signal that the plan is on track.
A decline across those markers is an early prompt to adjust training load, nutrition, or recovery — well before symptoms or standard health markers signal a problem.
A mix of rising and declining markers might indicate that you are, for example, doing well in your HYROX training but not as optimised in your long-term health.
The list of examples goes on depending on your preferred lifestyle and exercise goals.
In the context of weight management, such a feedback loop is useful to point you in the right direction.
7. It Can Surface Issues Worth a Medical Conversation
My company’s lactate threshold test requires you to produce a maximal effort, and that can sometimes reveal something worth following up on:
an unusual heart rate response
symptoms of cardiac irregularity
unexpectedly low fitness for age
Etc.
While such cases may not be entirely related to weight management, these observations can prompt a timely conversation with a physician or cardiologist.
Conclusion
With everything said, it is key to note that perimenopausal symptoms — hot flushes, sleep disruption, mood changes, brain fog — and any decisions about hormone therapy belong in a clinical conversation with a doctor.
My company’s metabolic profiling, while advanced, provides no guidance on these, despite some clients asking.
Lastly, I want to point out that the research base for training prescriptions specific to perimenopausal and postmenopausal women is still developing.
This article will be updated for accuracy if new evidence emerges.
These limitations aside, if you have any questions on the topic, please get in touch.
For more of such content, consider subscribing to the newsletter.
Till next time, take care!
References
Abildgaard, J., Pedersen, A. T., Green, C. J., Harder-Lauridsen, N. M., Solomon, T. P. J., Thomsen, C., Juul, A., et al. (2013). Menopause is associated with decreased whole body fat oxidation during exercise. American Journal of Physiology-Endocrinology and Metabolism, 304(11), E1227–E1236. https://doi.org/10.1152/ajpendo.00492.2012
Carter, S. L., Rennie, C., & Tarnopolsky, M. A. (2001). Substrate utilization during endurance exercise in men and women after endurance training. American Journal of Physiology — Endocrinology and Metabolism, 280(6), E898–E907. https://doi.org/10.1152/ajpendo.2001.280.6.E898
Fleg, J. L., Morrell, C. H., Bos, A. G., Brant, L. J., Talbot, L. A., Wright, J. G., & Lakatta, E. G. (2005). Accelerated longitudinal decline of aerobic capacity in healthy older adults. Circulation, 112(5), 674–682. https://doi.org/10.1161/CIRCULATIONAHA.105.545459
Greendale, G. A., Sternfeld, B., Huang, M., Han, W., Karvonen-Gutierrez, C., Ruppert, K., Cauley, J. A., Finkelstein, J. S., Jiang, S.-F., & Karlamangla, A. S. (2019). Changes in body composition and weight during the menopause transition. JCI Insight, 4(5), e124865. https://doi.org/10.1172/jci.insight.124865
Iannetta, D., Inglis, E. C., Mattu, A. T., Fontana, F. Y., Pogliaghi, S., Keir, D. A., & Murias, J. M. (2020). A critical evaluation of current methods for exercise prescription in women and men. Medicine & Science in Sports & Exercise, 52(2), 466–473. https://doi.org/10.1249/MSS.0000000000002147
Ioannidou, P., Dóró, Z., Schalla, J., Wätjen, W., Diel, P., & Isenmann, E. (2024). Analysis of combinatory effects of free weight resistance training and a high-protein diet on body composition and strength capacity in postmenopausal women — A 12-week randomized controlled trial. The Journal of Nutrition, Health & Aging, 28(11), 100349. https://doi.org/10.1016/j.jnha.2024.100349
Isacco, L., Duché, P., & Boisseau, N. (2012). Influence of hormonal status on substrate utilization at rest and during exercise in the female population. Sports Medicine, 42(4), 327–342. https://doi.org/10.2165/11598900-000000000-00000
Isacco, L., & Boisseau, N. (2021). Sex hormones and substrate metabolism during endurance exercise. In: Hackney A.C., Constantini N.W. (eds), Endocrinology of Physical Activity and Sport. Humana, Cham. https://doi.org/10.1007/978-3-030-33376-8_11
Kodama, S., Saito, K., Tanaka, S., Maki, M., Yachi, Y., Asumi, M., et al. (2009). Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: A meta-analysis. JAMA, 301(19), 2024–2035. https://doi.org/10.1001/jama.2009.681
Loe, H., Rognmo, Ø., Saltin, B., & Wisløff, U. (2013). Aerobic capacity reference data in 3,816 healthy men and women 20–90 years. PLOS ONE, 8(5), e64319. https://doi.org/10.1371/journal.pone.0064319
Lovejoy, J. C., Champagne, C. M., de Jonge, L., Xie, H., & Smith, S. R. (2008). Increased visceral fat and decreased energy expenditure during the menopausal transition. International Journal of Obesity, 32(6), 949–958. https://doi.org/10.1038/ijo.2008.25
Mader, A., & Heck, H. (1986). A theory of the metabolic origin of ‘anaerobic threshold.’ International Journal of Sports Medicine, 7(S1), S45–S65. https://doi.org/10.1055/s-2008-1025802
Mandsager, K., Harb, S., Cremer, P., Phelan, D., Nissen, S. E., & Jaber, W. (2018). Association of cardiorespiratory fitness with long-term mortality among adults undergoing exercise treadmill testing. JAMA Network Open, 1(6), e183605. https://doi.org/10.1001/jamanetworkopen.2018.3605
Ponce-González, J. G., et al. (2018). Reduced fat oxidation during exercise in post-menopausal overweight-obese women with higher lipid accumulation product index. Medicine, 97(18), e0557.
Randle, P. J., Garland, P. B., Hales, C. N., & Newsholme, E. A. (1963). The glucose fatty-acid cycle: Its role in insulin sensitivity and the metabolic disturbances of diabetes mellitus. The Lancet, 281(7285), 785–789. https://doi.org/10.1016/S0140-6736(63)91500-9
Tarnopolsky, L. J., MacDougall, J. D., Atkinson, S. A., Tarnopolsky, M. A., & Sutton, J. R. (1990). Gender differences in substrate for endurance exercise. Journal of Applied Physiology, 68(1), 302–308. https://doi.org/10.1152/jappl.1990.68.1.302
Venables, M. C., Achten, J., & Jeukendrup, A. E. (2005). Determinants of fat oxidation during exercise in healthy men and women: A cross-sectional study. Journal of Applied Physiology, 98(1), 160–167. https://doi.org/10.1152/japplphysiol.00662.2003
Vogel, B., Acevedo, M., Appelman, Y., Bairey Merz, C. N., Chieffo, A., Figtree, G. A., et al. (2021). The Lancet women and cardiovascular disease Commission: Reducing the global burden by 2030. The Lancet, 397(10292), 2385–2438. https://doi.org/10.1016/S0140-6736(21)00684-X